



This article has been provided by Dr. Huseyin ACAR to give information about ‘Lacrimal Outflow System Obstruction in Children’ in general terms.
WHAT IS THE STRUCTURE OF LACRIMAL OUTFLOW SYSTEM ?
Tear (or lacrima) is excreted by the lacrimal gland located at the upper part of our eyes. After it completes its function, it leaves the eye from the holes located at the upper and lower eyelids and then tear enters into the channel system. This channel system is mainly consisted of 6 parts: the first part is the holes. The holes exist at the upper and lower sections of the eyelids’ internal corners nearby the nose. They are not seen from outside but can be observed in case the eyelids are lifted towards outside. Lacrima enters into the channel system throughout these holes. The second part is the canaliculus. Lacrima is transferred into lacrimal sac via these canaliculi. Afterwards it passes into the nasal cavity via lacrimal duct.
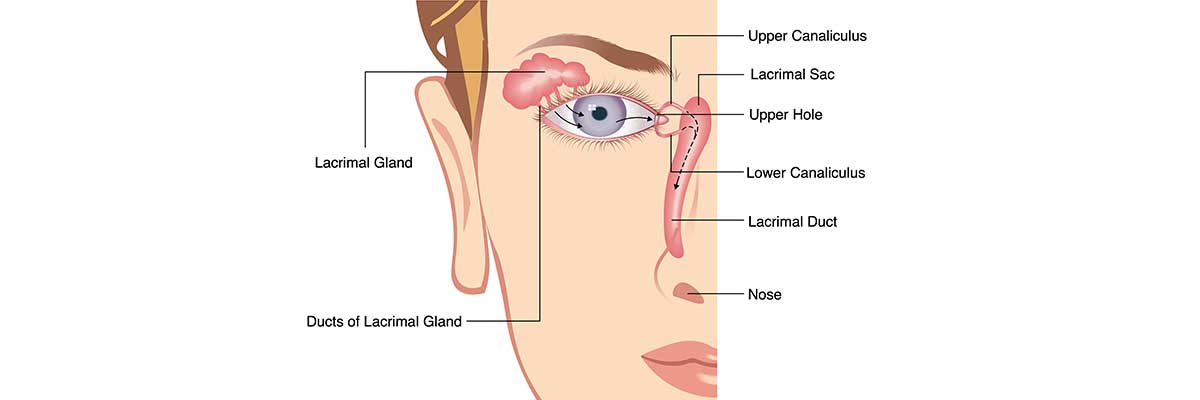
Image 1: Anatomy of tear outflow system
WHAT ARE CAUSES AND SYMPTOMS OF LACRIMAL DUCT ONSTRUCTION IN CHILDREN ?
Development of lacrimal duct system is usually completed before the birth. However, this formation is not completed for some babies and an obstruction occur in the lacrimal duct of the child. In such cases, it is observed that there is the tearing and the secretion in the eyes.
WHAT IS THE TREATMNET OF LACRIMAL DUCT OBSTRUCTION IN CHILDREN ?
Generally such patients have been followed up for a while since there is a high chance of self-treatment of lacrimal duct obstruction in children. During such follow up, massaging on the lacrimal sac may increase the chance to open the duct. The most important issue is the infection risk. Patients having obstruction in the duct tend to have eye infections. Thus, an additional care for the hygiene of eye lid should be taken. The formed secretion should be cleaned by a clean swap with the help of warm water or by a handkerchief specifically manufactured for such purposes sold in the pharmacies. In case of probable infection situation, eyes become red and yellow colored secretion turns into green color. During such periods, patients are treated by the antibiotic drops or ointment. However it is revealed by the researches that usage of pharmaceuticals does not decrease the risk of infection and on the contrary it leads to resistance of microorganism against the drugs used when there is no infection. Generally accepted opinion about intervention time is around 1 year of the baby although there are different opinions about this timing. Interventions taken after one and the half years old have less success rate. Intervention can be done earlier for the patients having eye infections frequently. Intervention usually is made under general anesthesia. After anesthesia, lacrimal outflow system of the child is examined and the level of obstruction is determined. After verification that obstruction is in the lacrimal duct, a stainless steel wire is inserted into the holes of lower and upper lids and obstructed area is opened. Success rate of the intervention is about 95%. The duct may obstruct again for some children, especially for the patients whom the intervention is not applied in time. In such cases, the same process is repeated but this time a silicon tube is installed into the system and remained it there for a while. A surgery for those patients who have not recovered sufficiently with this second method is applied to open a new duct.
SUMMARY
Lacrimal duct obstruction in children is formed due to the delay in the development of lacrimal duct system. In the most patients, this obstruction is spontaneously opened after the birth within one year period. Chances of recovery can be increased by massaging to the lacrimal sac during this period. The most important issue in this period is the infection risk. The best measure against the infections is to clean the eyelids regularly. Timing of the intervention is the crucial one because delay in the intervention decreases the success rate.